How the Patient Found the Practice
The patient was referred to Dr. Pytlik by their general dentist. The patient had been wearing partials for the longest time and wanted to have implants placed.
The general dentist recognized that the patient had a collapsed bite and needed their bite’s vertical dimension opened before implants were placed.
This referral demonstrates sophisticated treatment planning by the referring dentist.
Many practitioners would proceed directly to implant placement in a patient requesting implants to replace missing posterior teeth.
However, the referring dentist understood that placing implants in an existing collapsed bite would compromise their long-term success and fail to address the underlying biomechanical problems causing the ongoing dental breakdown.

Pre-treatment retracted view with teeth separated showing extent of tooth loss and dental breakdown. Visible gaps in posterior regions and compromised anterior teeth. Collapsed bite evident from reduced vertical dimension and anterior overload pattern.
Initial Condition & Life Before Treatment
The patient was advised that his teeth were fractured and misaligned, and because he was lacking back lower teeth, he was overloading his front teeth in both the lower arch and the upper arch.
This caused fracturing. The patient admitted to not being able to wear lower partials due to them being unstable and constantly pinching.
This clinical presentation illustrates a common cascade of failure in patients with posterior tooth loss.
When posterior teeth are missing, the anterior teeth must bear chewing forces they were never designed to handle. Posterior teeth have large, broad occlusal surfaces and multiple roots specifically designed to absorb and distribute heavy masticatory forces.
Anterior teeth, by contrast, have small incisal edges and single roots, designed primarily for tearing food and guiding jaw movements rather than sustaining heavy chewing loads.
When a patient loses posterior support and attempts to compensate by chewing on anterior teeth, several predictable problems occur. The excessive forces cause the anterior teeth to fracture, wear, or loosen. The bite collapses as posterior teeth are lost and anterior teeth tip or drift.
The mandible rotates upward and forward, further compromising the occlusion. Eventually, even the remaining anterior teeth begin to fail under the abnormal loading.
Removable partial dentures are often prescribed to replace missing posterior teeth, but they frequently fail to provide adequate function.
The patient’s experience of instability and constant pinching is typical. Lower partial dentures, in particular, are notoriously difficult to stabilize due to the mobile nature of lower arch soft tissues and the reduced denture-bearing area compared to the upper arch.
Patients often find them uncomfortable, remove them for eating (defeating their purpose), and eventually abandon them entirely.
First Appointment & Discovery
At the first appointment, the patient was evaluated for lower arch dental implants. However, the patient understood that he needed to have his teeth redone prior to planning the surgery.
This represents a critical insight into treatment sequencing.
While the patient presented requesting implants, Dr. Pytlik recognized that successful implant treatment required first addressing the collapsed bite and failing dentition. Attempting to place implants without first correcting the occlusion would be attempting to build on an unstable foundation.
The comprehensive workup for lower arch dental implants at the initial appointment served multiple purposes.
It demonstrated to the patient that Dr. Pytlik was taking his implant goals seriously and had a clear plan to achieve them.
It also established the treatment goal, creating a roadmap to guide all subsequent decisions.
Most importantly, it allowed Dr. Pytlik to plan backward from the ideal final implant position to determine what the restorative work needed to accomplish.
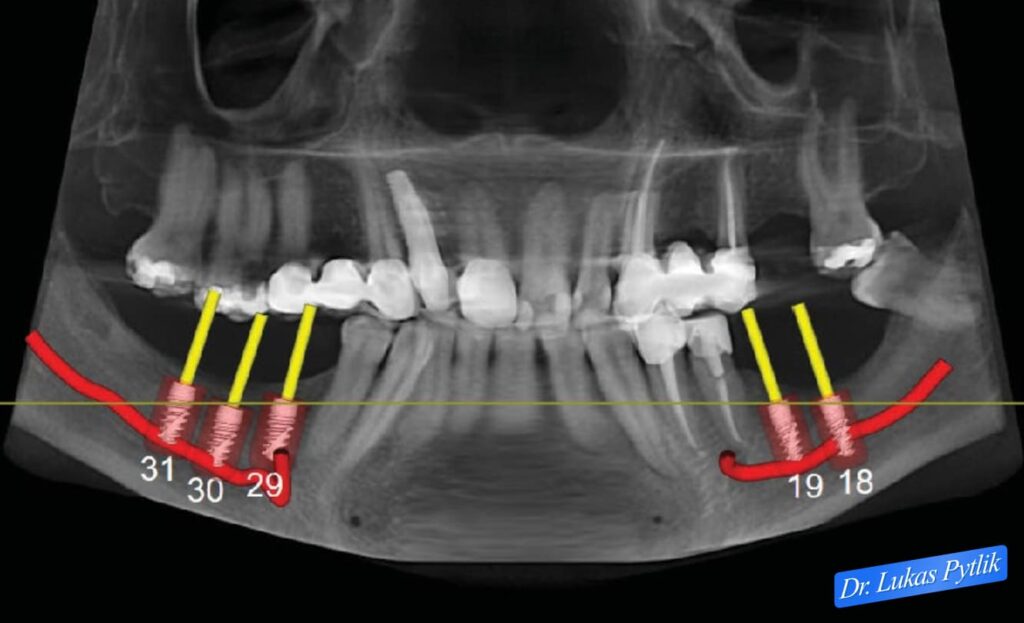
Pre-treatment panoramic radiograph with digital implant planning overlay. Yellow markers indicate planned implant positions in lower posterior regions (positions 18, 19, 29, 30, 31). Red curved lines indicate areas of significant bone loss that require strategic implant positioning.
Misunderstandings or Clinical Oversights
Some patients or dentists do not realize that, for ideal implant placement and long-term success, the restoration plan must begin by idealizing the final restoration’s position.
In this case, the patient understood that once the teeth were crowned and the final implant crowns were in place, the surgeon could be given the exact trajectory for implant placement.
This represents a fundamental principle of implant dentistry that is often overlooked: implants should be placed restoratively, not surgically driven.
The question should never be “where can we place an implant given the available bone?” but rather “where does the implant need to be to support an ideal restoration?”
When implants are placed solely for surgical convenience or based on available bone without reference to the final restoration, the result is often an implant that emerges through the occlusal surface at an unfavorable angle, requires excessively angled abutments, creates cantilevers, or positions the restoration in a biomechanically compromised relationship with opposing teeth.
The proper sequence is to first establish ideal occlusion with provisional or final restorations on the remaining natural teeth, then use that ideal occlusion to determine precisely where implant-supported crowns should be positioned, and finally use surgical guides to place implants in the exact three-dimensional position to support those crowns.
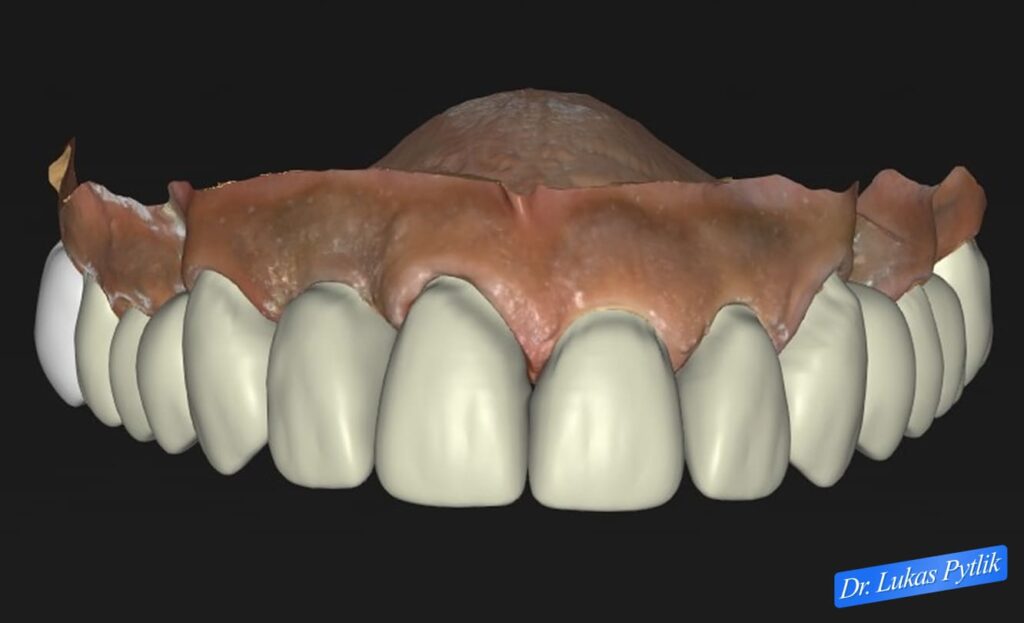
Digital treatment design showing frontal view of planned maxillary restoration.
This approach requires collaboration between the restorative dentist and the surgeon, with the restorative dentist leading treatment planning.
The restorative dentist determines the ideal position and angulation of the future implant crown, and the surgeon uses this information (typically provided via a surgical guide) to place the implant fixture in the precise position needed to support that restoration.
Treatment Plan & Approach
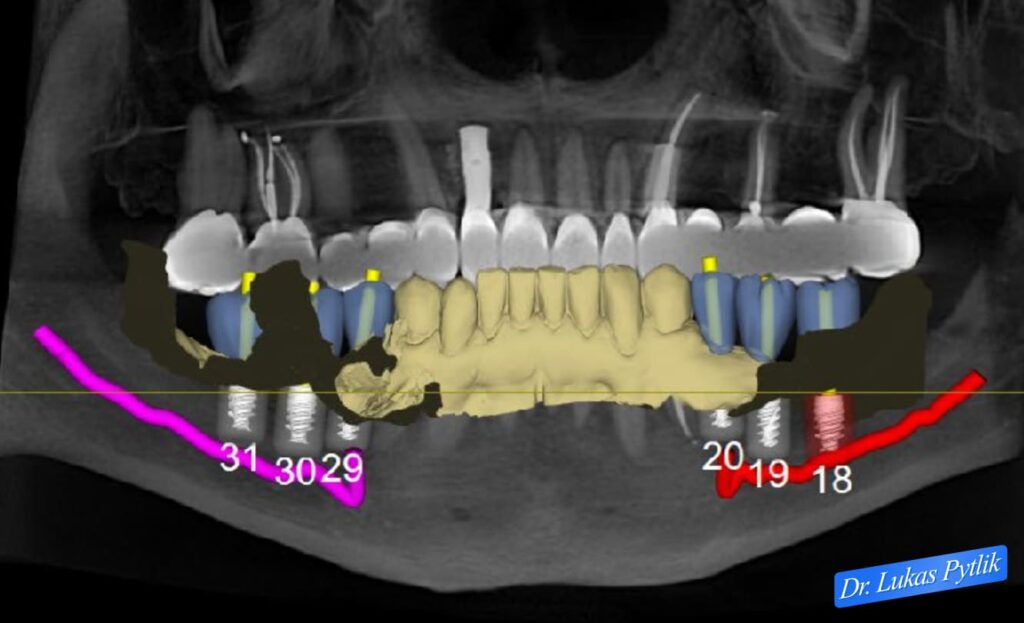
Post-rehabilitation panoramic radiograph showing completed restorative work with digital overlay of planned implant positions. Note that implant planning now references the established ideal occlusion from the completed crown-and-bridge work.
The patient underwent full mouth rehabilitation.
At the first appointment, all maxillary upper teeth were prepared for new crowns and bridges, and then temporized with ideal crowns to the patient’s liking.
At the second appointment, the lower teeth were temporized after preparation for crowns.
At the third appointment, the patient received final restorations in the color he chose with his wife.
This staged approach serves multiple clinical purposes. By treating the upper arch first, Dr. Pytlik established a stable reference plane against which to develop the lower arch occlusion. The upper arch typically provides a more stable platform for establishing occlusal relationships, as it is less susceptible to functional and parafunctional forces that often compromise the lower arch dentition.
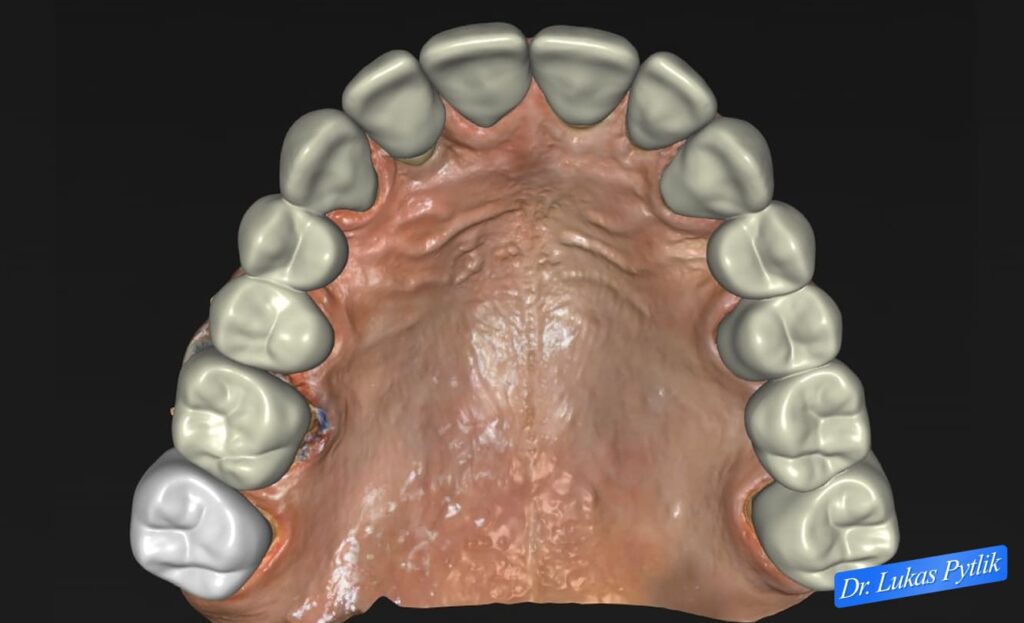
Overhead view of digitally planned maxillary restoration showing ideal occlusal anatomy and contact relationships.
The provisional phase is particularly critical in cases involving changes in vertical dimension and extensive reconstruction.
The temporaries allowed the patient to adapt to the new bite height, verified that the vertical dimension increase was comfortable and sustainable, and provided a “blueprint” of the final restoration that both doctor and patient could evaluate before committing to definitive materials.
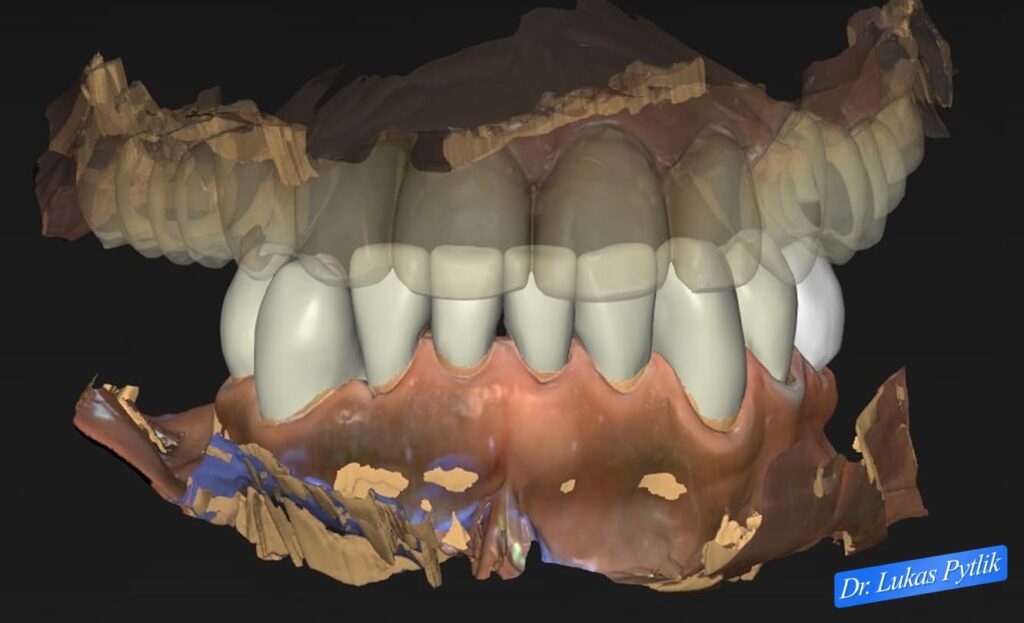
Digital design of mandibular restoration in frontal view showing planned crown coverage and anterior aesthetics. Lower arch design coordinates with upper arch restoration to create harmonious occlusal relationships at corrected vertical dimension.
The patient also chose to have an acrylic partial and night guards placed on his teeth.
The acrylic partial provided some posterior support during the restorative phase and served as a transitional appliance until implants could be placed and restored.
The night guard protected the new restorations from excessive forces during nocturnal bruxism, a critical consideration in any extensive restorative case.
The patient was evaluated for implants, and surgical guides were fabricated for placement.
These surgical guides were created using the information from the completed full-mouth rehabilitation. With the ideal occlusion now established, Dr. Pytlik could determine precisely where the implant-supported crowns needed to be positioned in the posterior regions.
The surgical guides translated this information into exact three-dimensional coordinates for implant placement, ensuring that when the surgeon placed the implants, they would emerge in the ideal position to support properly contoured and angled crowns.
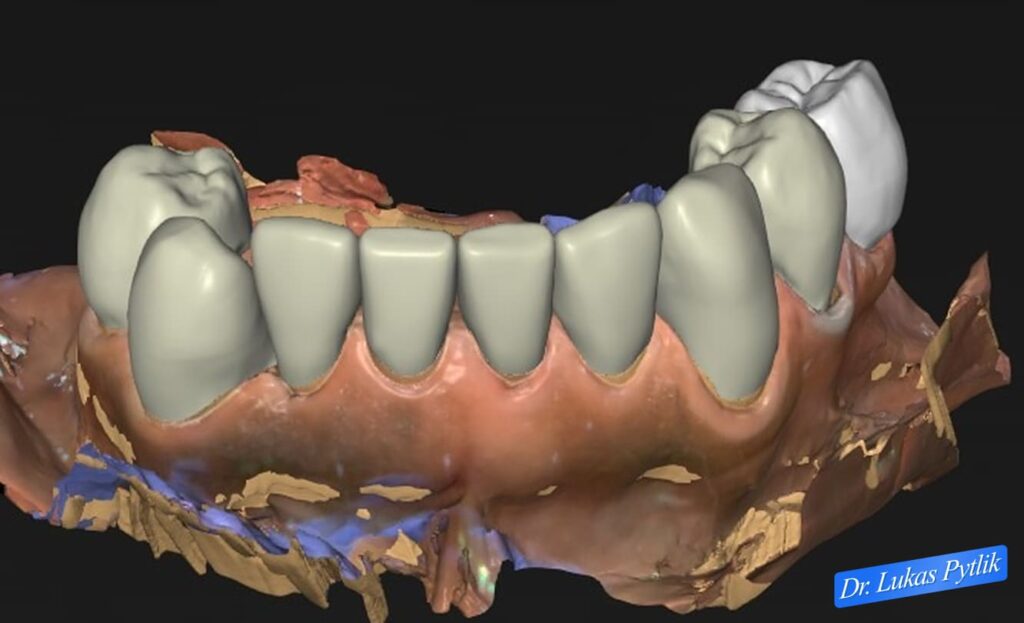
Overhead digital view of planned mandibular restoration showing comprehensive crown coverage and ideal occlusal surfaces. Design accounts for missing posterior teeth that will later be replaced with implant-supported crowns following guided surgical placement.
Case Progression & Key Milestones
The patient loved the esthetics of his new crowns and felt himself smiling more than ever.
The patient was very confident about wearing his partial. However, he knew that, for him to chew properly and eat all the foods he had been missing, he needed implants.
This emotional response reflects the transformative impact of restoring anterior esthetics. Even though the functional goals of treatment (restoring chewing ability through posterior implants) had not yet been achieved, the aesthetic improvement alone dramatically improved the patient’s confidence and quality of life.
The patient’s awareness that the treatment was not yet complete and that he still needed implants to achieve full function demonstrates successful patient education.
He understood that the comprehensive rehabilitation was a staged process with clear milestones, and he remained committed to completing treatment even though significant improvement had already been achieved.
The patient was worked up for lower right implants and two lower left implants due to the bone loss in the lower back area of his jaw.
The specific number and placement of implants were determined by the available bone and the number of teeth to be replaced. The asymmetric approach (different numbers of implants on each side) reflects individualized treatment planning based on the patient’s specific anatomy and needs rather than a one-size-fits-all protocol.

Natural smile photograph showing completed aesthetic outcome. Patient displaying confident smile with proper tooth proportions and natural appearance. Restoring the vertical dimension improves facial aesthetics and tooth display during smiling.
Outcome
Clinical Outcome
The patient is currently going through healing after implant placement, which went very predictably.
The surgical phase proceeded without complications, reflecting the benefits of thorough planning and surgical guides for precise implant positioning.
The healing phase following implant placement typically requires several months to allow for osseointegration, the process by which the titanium implant surface integrates with the surrounding bone. During this time, the patient continues to wear the acrylic partial for posterior support and esthetics.
Once osseointegration is complete, the implants will be uncovered and restored with final implant-supported crowns. These crowns will be designed to fit harmoniously with the comprehensive rehabilitation already completed on the natural teeth, creating a unified occlusal scheme that distributes forces appropriately across all teeth and implants.
The patient and his wife were very happy with the esthetic outcome of his crowns.
The collaborative approach to shade selection, with the patient’s wife involved in the decision-making, ensured the final result met the expectations of both partners.
The aesthetic improvement extended beyond just the appearance of individual teeth.
By correcting the collapsed bite and restoring proper vertical dimension, Dr. Pytlik improved the patient’s facial proportions and smile dynamics.
Patients with collapsed bites often appear older than their years due to reduced lower facial height and less tooth display during smiling. Restoring vertical dimension can have a rejuvenating effect on facial appearance.
The patient is extremely eager to have his implant crowns restored, so his case is complete and he can start eating the foods he has been unable to eat for the past few years.
This anticipation reflects the patient’s understanding of what full treatment completion will achieve.
While the aesthetic improvements have been immediately gratifying, he recognizes that the functional restoration provided by the posterior implants will be truly life-changing.
The ability to eat a full range of foods without pain, difficulty, or anxiety about dislodging a partial denture represents a fundamental improvement in quality of life.
The patient’s journey from someone experiencing progressive dental failure, unable to wear partial dentures comfortably, and limited in food choices, to someone with a restored smile and anticipating full chewing function, illustrates the comprehensive impact of well-planned prosthodontic care.
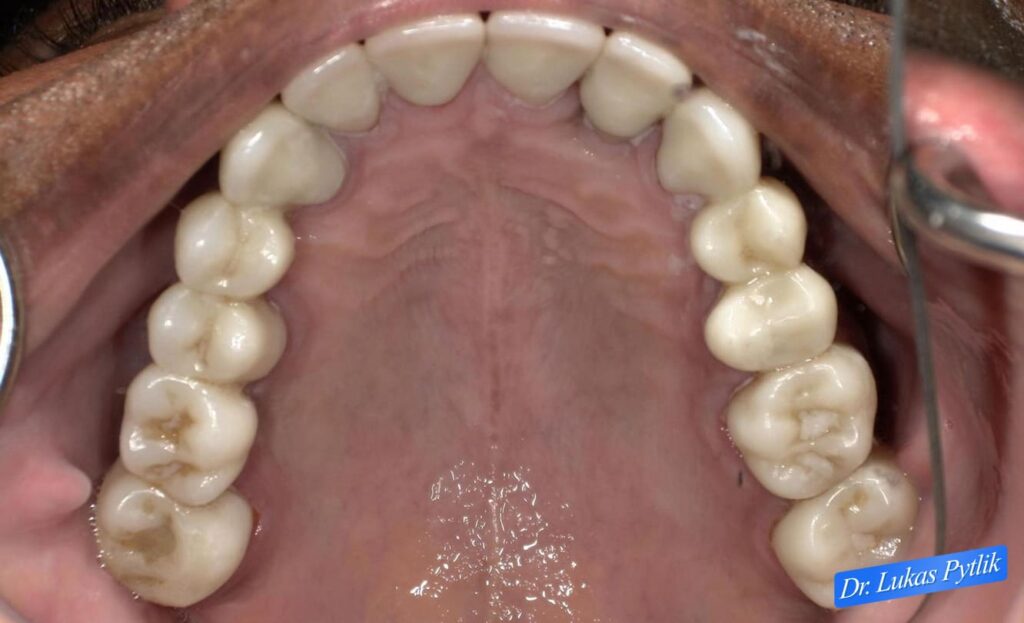
Clinical photograph showing completed maxillary restoration from occlusal perspective. Comprehensive crown coverage with proper contours and contact relationships. Ideal occlusal surfaces established throughout arch.
Treatment Time, Start to Finish
The patient had three treatment appointments and one delivery appointment for the restorative phase. This efficient timeline reflects systematic treatment planning and execution.
The implant phase is underway, with implants placed and healing in progress before the crowns are restored.
Clinical Notes for Referring Doctors
This case demonstrates a highly successful approach to converting a patient who is very unhappy with a collapsed bite and fractured teeth into a highly compliant patient who takes great accountability for his teeth and hygiene.
Key clinical considerations in this case included:
Restoratively-Driven Implant Planning: The fundamental principle demonstrated in this case is that implant position must be determined by the ideal restoration position, not by surgical convenience.
By completing the full-mouth rehabilitation first and establishing ideal occlusion, Dr. Pytlik created a roadmap for precise implant placement. Surgical guides fabricated from this ideal occlusion ensure that implants are positioned to support properly contoured and angled crowns.
Treatment Sequencing: The sequence of (1) comprehensive occlusal rehabilitation, (2) implant surgery with guided placement, and (3) final implant crown restoration ensures that each phase builds logically on the previous phase.
Attempting to shortcut this sequence by placing implants before establishing proper occlusion compromises the entire treatment.
Addressing Root Causes: Rather than simply replacing missing teeth with implants in an existing collapsed bite, this treatment addressed the underlying biomechanical problems.
The collapsed bite was opened, the fractured teeth were restored, and only then were implants placed into a corrected occlusal scheme.
Patient Education and Engagement: The patient’s transformation from someone experiencing progressive failure to someone taking accountability for their oral health reflects the success of patient education.
By involving the patient in treatment planning, explaining the rationale for each phase, and demonstrating results progressively, Dr. Pytlik created an engaged partner in treatment rather than a passive recipient.
Provisional Restoration Phase: The use of comprehensive provisional restorations served multiple critical functions: verifying vertical dimension changes, allowing neuromuscular adaptation, providing a blueprint for final restorations, and guiding implant position planning.
Staged Functional Restoration: The use of an acrylic partial denture during the restorative and implant-healing phases provided interim posterior support while the definitive solution (implant-supported crowns) was being developed.
This prevented overloading of the newly restored anterior teeth during the transitional period.
This case is appropriate for referral when patients present with: posterior tooth loss causing a collapsed bite and anterior overloading; fractured or failing teeth from biomechanical overload; unsuccessful partial denture treatment; or complex cases requiring coordination of comprehensive restorative work with strategic implant placement.
Dr. Pytlik welcomes referrals for complex prosthodontic cases requiring full mouth rehabilitation, vertical dimension management, and coordinated implant planning with surgical guide fabrication.