Patient Testimonial
“I love my new natural smile. I love how my upper teeth show when I talk and smile.”
How the Patient Found the Practice
The patient found Dr. Pytlik’s practice because it is in-network with her insurance.
This demonstrates that high-quality specialty prosthodontic care can be accessible within insurance networks, allowing patients to receive expert treatment while managing their healthcare investment.
Initial Condition & Life Before Treatment
The patient had seen multiple dentists to restore her front teeth without success. Every time restorations in the interior maxillary arch were placed, they would come loose due to the bite issue.
The initial photographs revealed that the patient’s restorations were very canted (buccally inclined) and loose.
This pattern of repeated restoration failure is a hallmark sign of underlying occlusal problems that must be addressed before successful long-term restoration can be achieved.
Simply replacing failed restorations without correcting the fundamental bite relationship creates a cycle of treatment and re-treatment, wasting both time and financial resources while leaving the patient frustrated and without functional dentition.
Class III skeletal malocclusion, commonly known as an underbite, occurs when the lower jaw is positioned forward relative to the upper jaw. This creates a reverse overjet, in which the lower anterior teeth are positioned in front of the upper anterior teeth.
In severe cases, this relationship forces upper anterior teeth to compensate by tipping outward (buccal inclination), attempting to meet the opposing lower teeth.
The patient also demonstrated significant wear on both the anterior and posterior teeth, indicating long-standing bruxism (teeth grinding).
When combined with class III malocclusion and collapsed vertical dimension, this created a perfect storm for restoration failure. The abnormal forces, unfavorable angles, and excessive grinding loads made it virtually impossible for conventional restorations to remain stable.

Pre-treatment lateral view showing limited tooth display during smile, gaps from missing restorations, and compromised aesthetics.

Post-treatment external smile showing dramatic improvement in tooth display.
First Appointment & Discovery
At the first appointment, the patient was advised that she had wear on her posterior and anterior teeth, and that there was not enough space in the anterior of her arch to accommodate full-size restorations.
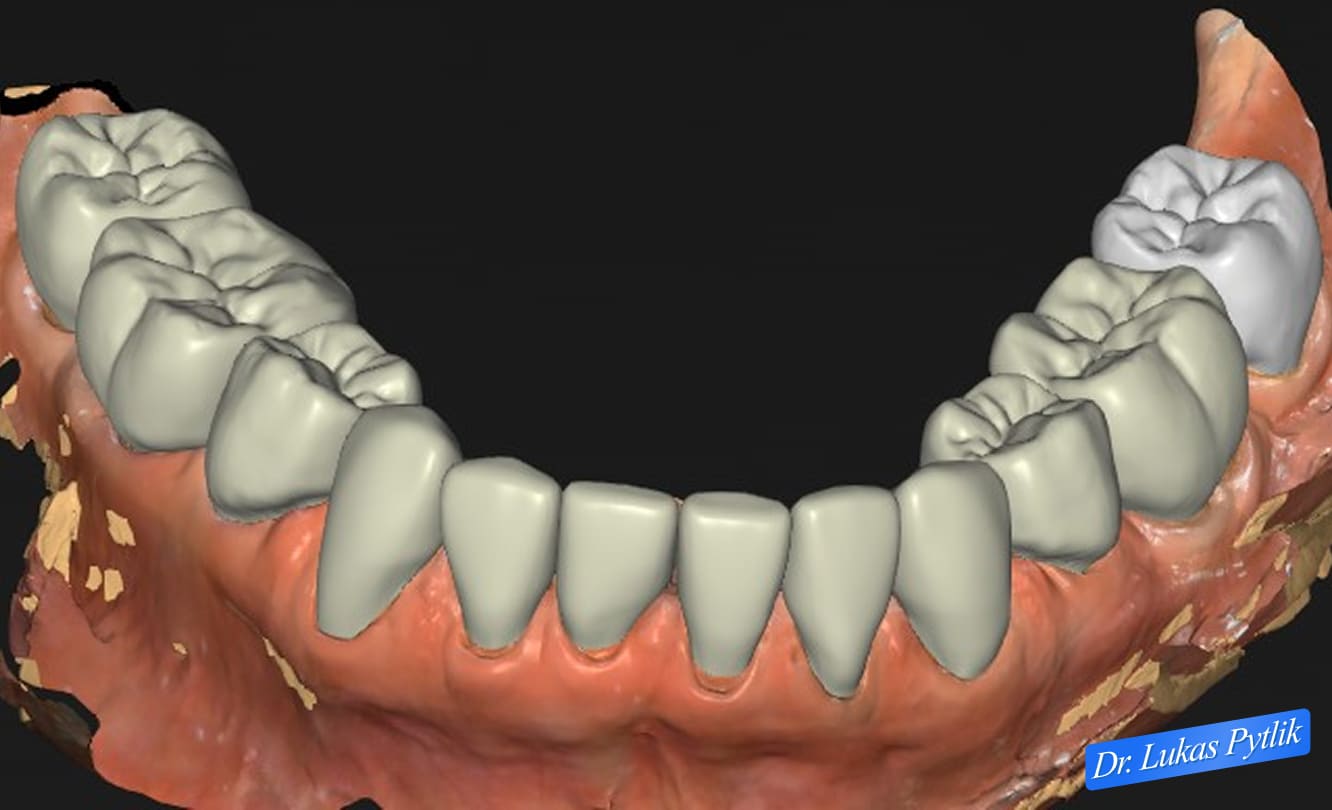
3D digital model showing existing dentition with worn posterior teeth and compromised anterior relationships.
The patient was counseled that, if she proceeded with full-mouth rehabilitation by increasing her vertical dimension, her front teeth would be less buccally inclined and would achieve a better esthetic result.
Vertical dimension refers to the height of the bite when the teeth are together. Over time, through grinding, wear, and tooth loss, this dimension can collapse, bringing the upper and lower jaws closer together.
This collapse has cascading effects throughout the entire dental system, affecting everything from tooth positioning to facial appearance to TMJ function.
By undergoing full-mouth rehabilitation, not only would her anterior teeth look better, but all her posterior teeth on the top and bottom would be restored with full-coverage crowns. This comprehensive approach is essential in cases like this because addressing only the anterior teeth while leaving worn posterior teeth would fail to achieve stable, long-term results.
Dr. Pytlik’s treatment philosophy emphasizes treating the entire masticatory system rather than individual teeth.
In complex cases involving skeletal malocclusion and vertical dimension loss, attempting to restore teeth in isolation generally leads to the kind of repeated failures this patient had already experienced with previous providers.
Misunderstandings or Clinical Oversights
In a class III skeletal occlusion case, when the vertical dimension collapses, it worsens the class III malocclusion (larger underbite). With a larger underbite, the patient will predominantly achieve greater occlusal contact on the anterior teeth.
This represents a critical concept that is often misunderstood or overlooked in general dentistry. Many practitioners see the underbite and buccally inclined anterior teeth as fixed anatomical features that must simply be worked around.
However, these relationships are dynamic and can be significantly improved by strategically manipulating the vertical dimension.
When the vertical dimension is lost, the mandible rotates upward and forward, exaggerating any existing class III tendency. This forward rotation places even more pressure on the anterior teeth, which must then tip further forward to maintain contact.
The result is a self-perpetuating cycle: bite collapse worsens the underbite, which increases anterior loading, which accelerates wear, which further collapses the bite.
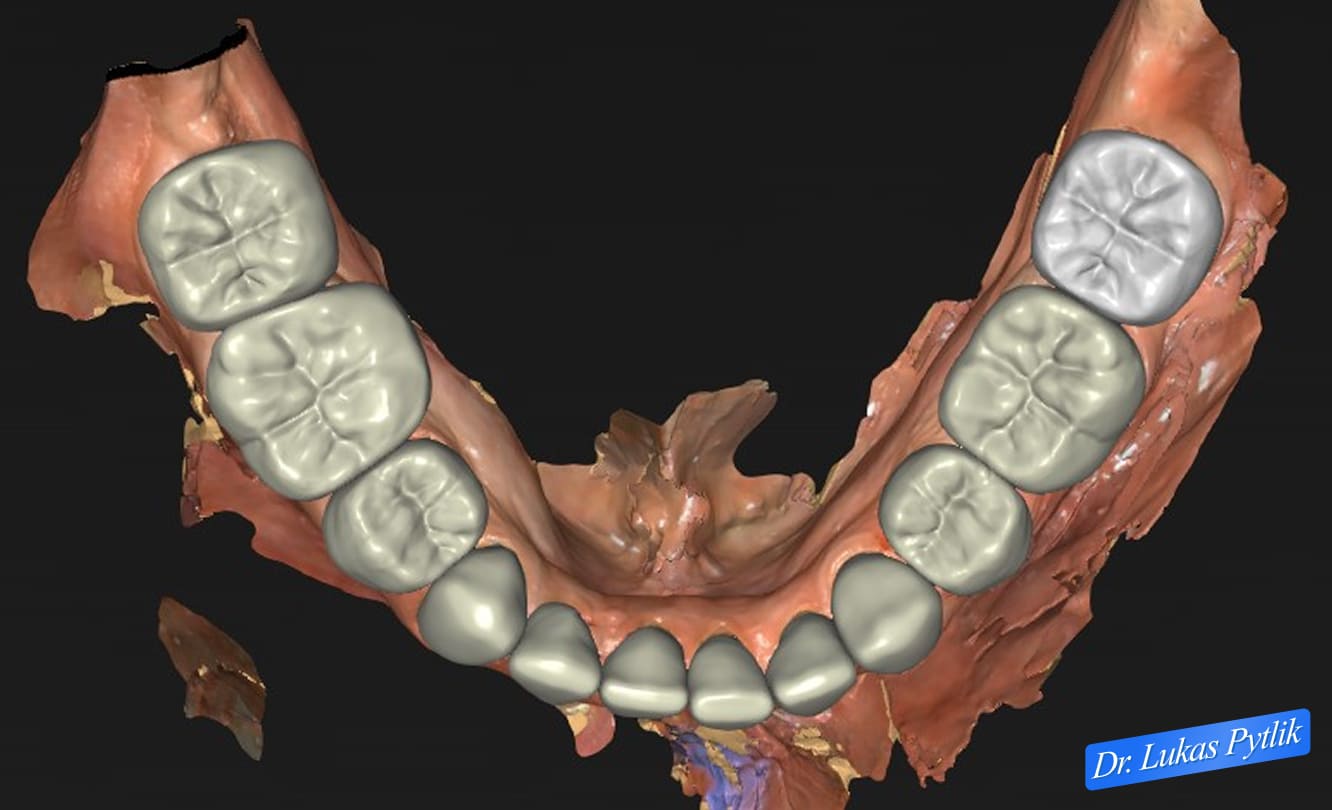
Mandibular arch showing worn occlusal surfaces and the need for full coverage restoration.
Understanding this relationship is fundamental to successful treatment. Simply replacing worn or broken anterior teeth at the existing collapsed vertical dimension dooms those restorations to the same failure pattern.
The restorations will be placed at unfavorable angles, will experience excessive occlusal forces, and will eventually fail, just as natural teeth and previous restorations have.
The solution requires comprehensive treatment that addresses the vertical dimension first, allowing for more favorable positioning of the anterior teeth and a more balanced force distribution throughout the arch.
Treatment Plan & Approach
By increasing the vertical dimension, the underbite is reduced, and the occlusion can be designed to primarily contact the posterior teeth. This fundamental principle drives the entire treatment approach: open the bite to improve the jaw relationship, then design restorations that distribute forces appropriately.
On day one, Dr. Pytlik idealized esthetics in the maxillary anterior teeth and posterior teeth.

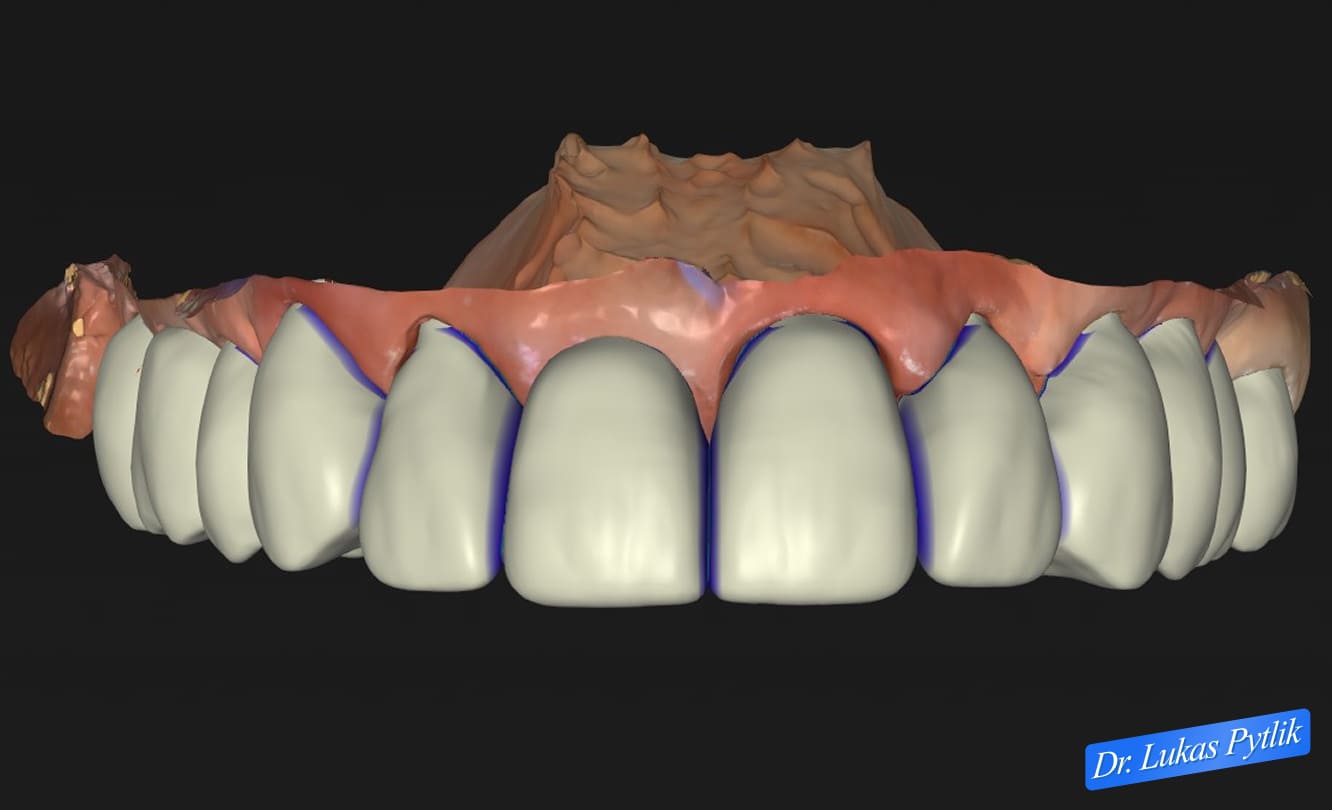
Computer-aided design of planned maxillary restorations showing increased vertical dimension and improved anterior tooth positioning.
On the second day, he idealized her esthetics and occlusion at an open vertical. After two days, the patient was very comfortable in her temporaries, and no temporaries came loose.
This provisional phase serves as critical proof of concept. The fact that temporary restorations remained stable even though previous definitive restorations repeatedly failed confirms that the treatment approach has successfully addressed the underlying problem.
The temporaries serve as a “test drive” of the new bite, allowing both the doctor and the patient to verify that the vertical dimension increase is comfortable, functional, and sustainable before committing to final restorations.
The comprehensive full-mouth rehabilitation included full-coverage crowns on all posterior teeth (upper and lower) and anterior restorations. By treating the entire dentition, Dr. Pytlik created a cohesive occlusal scheme where forces are distributed evenly across all teeth rather than concentrated in a few vulnerable areas.
Strategic planning of the new occlusion ensured that the posterior teeth would bear the primary chewing loads, while the anterior teeth would serve their proper role of guiding jaw movements and supporting facial esthetics.
This represents the ideal functional arrangement that protects both restorations and natural tooth structure.
The patient still needed to address her bruxism with Botox injections and a night guard to prevent any loosening of crowns or breaking of teeth.
While the improved occlusion significantly reduces destructive forces during normal function, nocturnal bruxism can still generate excessive loads. Combining Botox to reduce muscle hyperactivity with a night guard to protect restorations provides comprehensive management of this ongoing concern.
Case Progression & Key Milestones
The patient loved the esthetics and appreciated the comprehensive approach to protecting her investment through bruxism management.
Treatment progressed smoothly through the provisional phase, with the patient experiencing immediate improvement in both function and appearance.
The stability of the temporary restorations throughout the provisional phase provided confidence that the final restorations would be successful. Unlike her previous experiences, where restorations would fail within weeks or months, these temporaries remained secure and comfortable throughout the treatment process.
The patient’s comfort and satisfaction during the temporary phase are a crucial milestone. It demonstrates not only that the treatment’s technical aspects are sound, but also that the patient has adapted well to the new vertical dimension and occlusal relationships.
Some patients require time to adjust to an increased vertical dimension, but the careful planning and execution of this case resulted in immediate comfort.
Treatment was completed in three treatment appointments, representing an efficient timeline for comprehensive full-mouth rehabilitation. This efficiency reflects Dr. Pytlik’s systematic approach and the advanced planning that allows complex cases to progress smoothly.
Outcome
The patient loves her full mouth rehabilitation. All restorations remain stable and secure, with no loosening or failures.
The improved occlusal relationship distributes forces appropriately, with posterior teeth bearing primary chewing loads and anterior teeth providing guidance and esthetics.
The patient is very confident that the crowns will not fall out now that her bite has been corrected. This psychological relief cannot be overstated. After years of repeated failures and the constant anxiety that accompanies unstable restorations, the patient now enjoys complete confidence in her dentition.
The comprehensive treatment addressed not only the immediate problem of failed restorations but also the underlying biomechanical issues that led to them. By correcting the vertical dimension and class III relationship, Dr. Pytlik created conditions for long-term success rather than simply replacing what had been lost.
The patient loves the color she chose and loves how natural the teeth look. By increasing her vertical dimension, more teeth are showing in her smile, and she cannot stop laughing and smiling when she sees family and friends.
This increased tooth display represents one of the most dramatic aesthetic benefits of vertical dimension restoration. As the bite collapses over time, less and less tooth structure is visible during smiling and speaking.
This creates an aged appearance and can make patients appear older than their actual years. By restoring proper vertical dimension, Dr. Pytlik achieved a rejuvenating effect that goes beyond simple tooth replacement.
The natural appearance of the restorations reflects careful attention to shade selection, morphology, and characterization. The patient was actively involved in color selection, ensuring that the final result matched her preferences and expectations.
By increasing her vertical dimension, more teeth show in her smile. The patient stated, “I love my new natural smile. I love how my upper teeth show when I talk and smile.”
This emotional transformation represents the true measure of successful prosthodontic treatment. Beyond clinical success metrics and objective functional improvements, the patient has experienced a profound increase in confidence and quality of life.
She is no longer anxious about restoration failure, no longer hiding her smile, and no longer avoiding social situations due to dental concerns.
The comprehensive treatment, addressing both functional problems (repeated restorative failures, poor occlusion) and aesthetic concerns (limited tooth display, compromised smile), delivered holistic improvement in the patient’s life.
Treatment Time, Start to Finish
Treatment was finished in three treatment appointments, representing an efficient timeline for comprehensive full-mouth rehabilitation. This streamlined approach reflects thorough treatment planning, precise execution, and Dr. Pytlik’s systematic protocols for complex restorative cases.
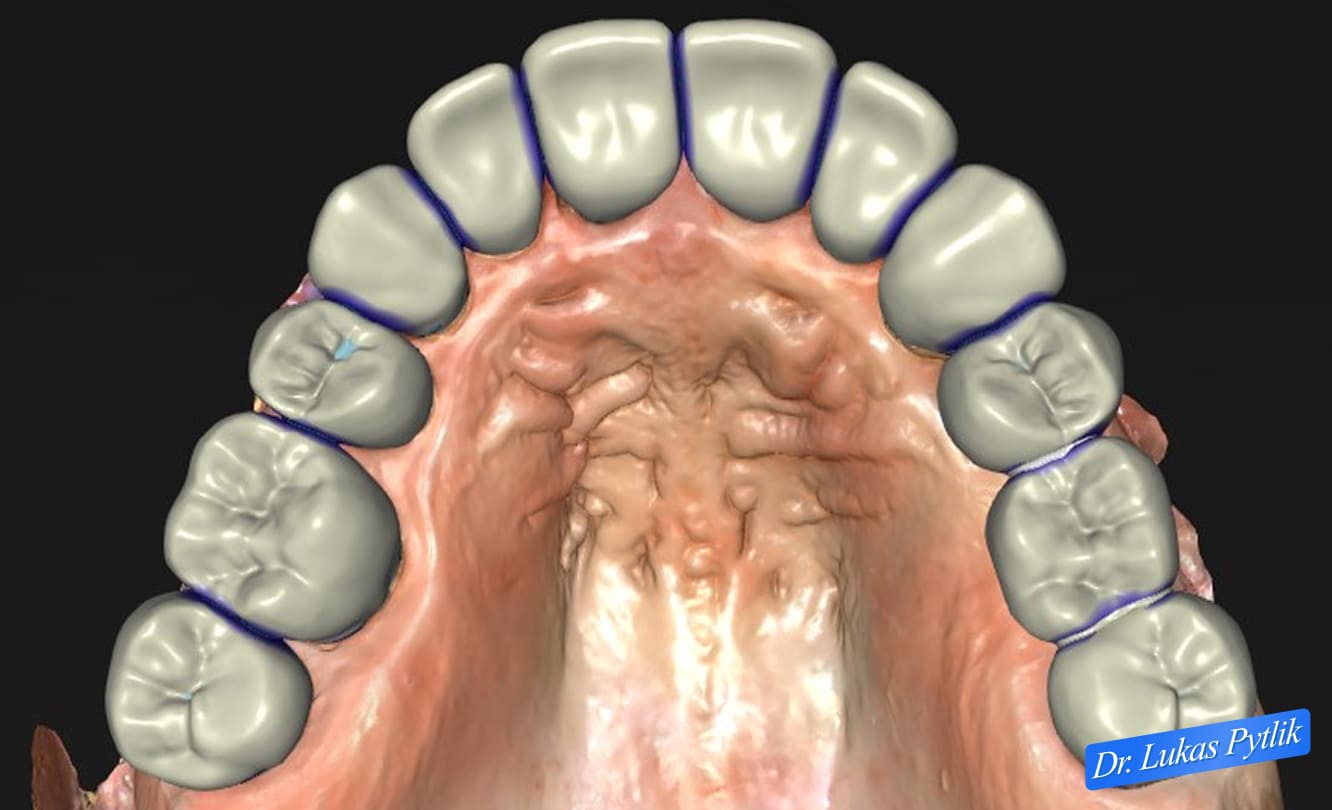
Overhead view of digitally planned restoration showing comprehensive crown coverage and optimized occlusal anatomy.
Clinical Notes for Referring Doctors
This case demonstrates the critical importance of recognizing and addressing underlying occlusal problems before attempting definitive restoration. The patient’s history of repeated restoration failures at multiple practices illustrates what happens when symptoms are treated without addressing root causes.
Key clinical considerations in this case included:
Vertical Dimension Assessment: The collapsed vertical dimension was a primary driver of both the aesthetic concerns and the mechanical restoration failures. Recognizing this relationship is essential in treatment planning for cases with significant wear or class III malocclusion.
Maxillary arch demonstrating wear patterns and restoration needs.
Class III Occlusion Management: In skeletal class III cases, bite collapse exacerbates the anteroposterior discrepancy. Strategic opening of the vertical dimension can significantly improve the jaw relationship without requiring orthognathic surgery.
This allows for more favorable positioning of anterior restorations and better force distribution.
Comprehensive vs. Segmental Treatment: Attempting to restore only the failing anterior teeth while leaving worn posterior teeth unaddressed would have perpetuated the unfavorable occlusal relationships.
Full mouth rehabilitation was necessary to achieve stable, long-term results.
Provisional Phase Validation: The stability of provisional restorations throughout treatment confirms that the biomechanical approach is sound. This “test drive” phase provides valuable information and builds patient confidence before the fabrication of the final restoration.
Bruxism Management: Even with optimal occlusion, patients with bruxism require protective strategies. The combination of improved occlusal design, night guard therapy, and adjunctive Botox treatment provides comprehensive management of parafunctional forces.
Treatment Efficiency: Complex full-mouth rehabilitation can be completed efficiently when proper planning and systematic protocols are employed. Three appointments for comprehensive upper and lower arch restoration represent streamlined care that respects patient time and resources.
This case is appropriate for referral when patients present with repeated restoration failures despite multiple treatment attempts, class III malocclusion with anterior compensation, significant wear with vertical dimension loss, or comprehensive rehabilitation needs requiring occlusal reorganization.
Dr. Pytlik welcomes referrals for complex prosthodontic cases requiring vertical dimension management, occlusal rehabilitation, and comprehensive arch restoration.