How the Patient Found the Practice
The patient found Dr. Pytlik’s practice through her parents. She lived in Los Angeles and was unable to get the care she needed from the restorative dentists there.
This highlights the challenges patients with complex conditions face when seeking appropriate care, often needing to travel significant distances to find a prosthodontist with the expertise to manage their unique combination of issues.
Initial Condition & Life Before Treatment
The patient came to Dr. Pytlik wanting a beautiful smile and to address her teeth, but she was apprehensive about crowning all her teeth and correcting her bite.
Initially, when the patient came in, she was biting only on her posterior teeth, with very light contact on the anterior front teeth.
The patient had temporomandibular disorder (TMD) with arthritis. Every time a restorative dentist placed a restoration in contact with the opposing arch, her bite would open, resulting in an open bite with contact only in the posterior.
This pattern represents a significant challenge in restorative dentistry.
TMD with active joint remodeling creates a moving target for occlusal design. When joints are inflamed or undergoing arthritic changes, the condylar position can shift, altering the relationship between upper and lower teeth.
Restorations that are in proper contact at the time of delivery may become out of contact as the joint remodels, or vice versa.
The open bite pattern, in which posterior teeth contact while anterior teeth do not, is a common manifestation of TMD. This unstable occlusal relationship makes it extremely difficult to maintain restorations in proper function, as forces and contacts constantly change with the status of joint inflammation.
Compounding these mechanical challenges, the patient suffered from severe dry mouth (xerostomia), likely medication-induced, combined with mouth breathing.
This created an environment highly conducive to dental decay, particularly cervical cavities (decay at the gum line).
Saliva plays a critical protective role in oral health, providing buffering capacity against acids, remineralization of early decay, and antimicrobial properties. Without adequate saliva, teeth become extremely vulnerable to rapid decay progression.
The patient was suffering from multiple cervical cavities around her teeth, which were darkening her teeth and causing black spots.
These cervical lesions not only caused functional problems but also significantly compromised the aesthetic appearance of her smile, resulting in visible dark areas at the gum line that were particularly noticeable when smiling or speaking.

Full face portrait demonstrating full mouth rehabilitation results, transforming tooth discoloration and cervical decay from medication-induced dry mouth and TMD to natural-looking smile with proper proportions and aesthetics.
First Appointment & Discovery
The patient was advised that her TMD and joint arthritis would cause continuous remodeling, creating ongoing changes in her interior region of the mouth.
Due to the patient’s severe dry mouth, she was suffering from multiple cervical cavities around her teeth, which were darkening her teeth and causing black spots. The patient was advised that, to protect the surfaces of her teeth, she would need to have all her teeth crowned and undergo full-mouth rehabilitation.

Retracted view with teeth in occlusion showing the extent of cervical decay and discoloration throughout the upper and lower arches.
This comprehensive approach serves multiple purposes in cases of severe xerostomia.
Full-coverage crowns protect vulnerable cervical areas (where the tooth meets the gum) from further decay by creating a sealed margin that is more resistant to the acid environment of dry mouth.
Additionally, porcelain or ceramic materials are less susceptible to decay than natural tooth structure, providing long-term protection even in the challenging oral environment created by medication-induced dry mouth.
The patient was offered gum surgery and orthodontics to align her gum lines. However, she refused because the gum irregularities were not visible in her smile when she was talking and smiling. The patient did not want to undertake any additional surgical procedures.
Crown lengthening surgery and orthodontic treatment could have created a more ideal gingival architecture and tooth positioning, potentially improving the aesthetic outcome.
However, patient autonomy in treatment decisions is paramount. Since the gum line irregularities were not visible in her natural smile line, the patient reasonably concluded that the additional time, discomfort, and cost of these procedures were not justified for her particular situation.
The patient understood that her crowns would look good when she talks and smiles, but if she lifted her lip, the crowns’ architecture would be very erratic; she wanted fewer surgeries and porcelain restoration to cover her roots.
This represents an important discussion about informed consent.
Dr. Pytlik ensured the patient had realistic expectations about the aesthetic result, acknowledging that while the smile would be beautiful in normal function, the underlying gum architecture would remain irregular.
This transparency allows patients to make fully informed decisions about their treatment.
The patient was advised and understood that if her TMD flares up and her bite in the interior opens up, an occlusal equilibration would be needed, in which the crowns would be adjusted so that all the teeth are touching.
This ongoing management strategy is crucial for TMD patients, as it acknowledges the condition’s dynamic nature and establishes a clear plan to address changes as they occur.
Misunderstandings or Clinical Oversights
Because the patient’s arthritis causes her temporomandibular joint to flare up, changing the occlusal position of the upper and lower teeth can adjust the bite, or crowns in the posterior region can be refabricated to allow a harmonious bite to return.
A common misconception in dentistry is that once final restorations are delivered, they should remain unchanged indefinitely. However, in patients with active TMD and joint remodeling, this expectation is unrealistic.
The biological changes in the joint create corresponding changes in occlusal relationships that must be managed over time.
The key insight is that these changes are manageable through periodic adjustments rather than requiring complete restoration or replacement.
By planning for this from the outset and educating the patient about the ongoing nature of TMD management, Dr. Pytlik established realistic expectations and a framework for long-term success.
Understanding that TMD is a chronic condition requiring ongoing management, rather than a problem that can be “fixed” once and for all, is essential for both practitioner and patient.
This case demonstrates how comprehensive prosthodontic treatment can be successful even in patients with active TMD when proper planning and patient education are employed.
Treatment Plan & Approach
The patient underwent a full-mouth rehabilitation procedure. On the first day, all her maxillary teeth were prepared for crowns, and temporaries were fabricated with a vertical dimension similar to her current condition.
On the second day, all the lower teeth were prepared for crowns and temporized at a comfortable vertical dimension.
This staged approach, treating upper and lower arches on separate days, allows for more controlled management of the occlusion. By establishing the maxillary arch first, Dr. Pytlik created a stable reference point against which to develop the mandibular occlusion. This is particularly important in TMD cases where the jaw position may be unstable.
Maintaining the existing vertical dimension rather than attempting to open or close the bite was a strategic decision based on the TMD diagnosis.
Significant changes to vertical dimension can potentially exacerbate TMD symptoms by altering the condylar position within the joint. By working within the patient’s existing comfortable vertical dimension, Dr. Pytlik minimized the risk of increasing joint stress.
The patient wanted to have the least amount of spaces between her teeth to prevent food impaction. The patient understood that her crowns would appear more square.
All the root surfaces were covered by porcelain.
Tighter contact areas between teeth reduce the likelihood of food trapping, which is particularly important for a patient with xerostomia, who already has an increased risk of decay. The trade-off is that square teeth create less interproximal space and tighter contacts than teeth with more rounded contours and visible embrasures.
Comprehensive coverage of all root surfaces with porcelain was essential, given the severe xerostomia.
The cervical cavities that had already developed demonstrated the vulnerability of these areas. By extending the crown margins to fully cover the root surfaces, Dr. Pytlik provided maximum protection against future decay in these high-risk areas.
On the third appointment, final restorations were cemented.
This efficient three-appointment protocol demonstrates a systematic approach that enables complex full-mouth rehabilitation to be completed within a reasonable timeframe.

Post-treatment retracted view with teeth in occlusion showing comprehensive crown coverage of both arches. All root surfaces are protected by porcelain.

Wide retracted view showing comprehensive upper and lower crown restorations in occlusion. All teeth are fully protected with porcelain coverage.
Case Progression & Key Milestones
The patient’s full mouth rehabilitation was extremely successful. She was pleased that she could finally go to brunches and events with her girlfriends without feeling self-conscious about her smile.
This social and emotional milestone often represents the true measure of success in aesthetic rehabilitation. The patient’s ability to participate fully in social activities without anxiety about her appearance transformed her quality of life beyond just the clinical improvements.
After a few months, when she noticed that the bite had opened up internally, the patient underwent a slight occlusal adjustment on the posterior upper and lower crowns to compensate for the TMD.
This follow-up adjustment demonstrates exactly what was discussed during treatment planning.
The TMD caused changes in joint position, resulting in an opening of the anterior bite. Rather than requiring a remake of the restorations, a simple adjustment to the posterior contacts reestablished proper occlusion across all teeth.
The patient’s understanding of this process and her acceptance of periodic adjustments as part of ongoing care are perfect examples of successful patient education.
Rather than viewing the need for adjustment as a treatment failure, she recognized it as an expected part of managing her chronic TMD condition.
Outcome
The patient was extremely happy with the final result of the full mouth rehabilitation. Her bite was very stable, and she was empowered by the idea that whenever she noticed a change, she only needed occlusal adjustments.
This sense of empowerment represents a crucial psychological outcome. Rather than feeling helpless in the face of a chronic condition, the patient understands she has a clear, straightforward solution available whenever adjustments are needed.
The predictability and simplicity of the management protocol provide peace of mind.
The comprehensive, full-coverage crowns successfully protect all tooth surfaces from further decay despite the ongoing challenge of severe xerostomia.
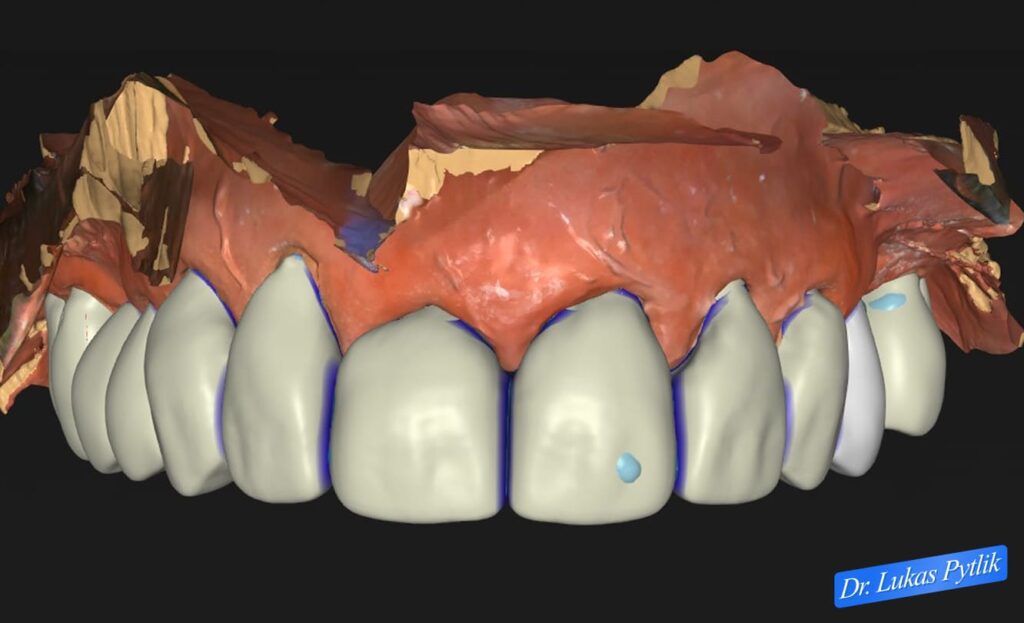
3D digital design of maxillary arch restoration showing planned crown contours with blue outline indicators. Design emphasizes comprehensive root coverage and protection of cervical areas vulnerable to xerostomia-related decay.
While the patient still needs to manage her dry mouth through other means (saliva substitutes, increased water intake, and a review of her medications with her physician), the teeth are now protected from the decay that had been progressively destroying them.
Even though the patient still had to manage her dry mouth, she thanked the office for the changes in her life since undergoing full-mouth rehabilitation.
The transformation extended beyond just the appearance of the teeth. The elimination of dark spots and discoloration at the gum lines, the comprehensive coverage of exposed root surfaces, and the creation of a cohesive, beautiful smile fundamentally changed how the patient presented herself to the world.
The aesthetic improvements were achieved while respecting the patient’s decision to forego additional surgical procedures.
This demonstrates that outstanding results can be accomplished through prosthodontic treatment alone when expectations are properly established and the limitations are clearly communicated.
The patient’s self-esteem and lifestyle have drastically changed. She could visit family, have lunch dates, and not have to worry about her smile.
This emotional transformation represents the most profound impact of successful prosthodontic treatment. The anxiety and self-consciousness that had been preventing full participation in social activities were eliminated.
The patient’s relationships, social life, and overall quality of life improved dramatically.
The patient’s multiple expressions of gratitude underscore the life-changing nature of this treatment. For someone who had been unable to find help in a major metropolitan area like Los Angeles, finding a solution that both addressed her complex clinical needs and delivered a beautiful aesthetic result was truly transformative.

3D digital model showing mandibular arch with existing dentition and planned restoration areas. Design reveals the extent of decay and the need for comprehensive, full-coverage restoration to protect vulnerable root surfaces from ongoing xerostomia effects.
Treatment Time, Start to Finish
Treatment was completed in three treatment appointments, demonstrating efficient management of a complex case involving both TMD considerations and extensive decay from xerostomia.

Complete digital case scan showing final design for both maxillary and mandibular full arch restorations. Comprehensive view of planned crown contours, occlusal relationships, and gingival architecture.
Clinical Notes for Referring Doctors
This case demonstrates the importance of managing patient expectations and empowering patients with chronic conditions through education and realistic treatment planning. The combination of active TMD with severe xerostomia creates significant challenges that require comprehensive prosthodontic intervention.
Key clinical considerations in this case included:
TMD Management in Full Mouth Rehabilitation: Patients with active TMD and joint remodeling require special consideration in treatment planning. Rather than viewing the dynamic nature of their occlusion as a contraindication to treatment, it should be recognized as a manageable condition requiring periodic adjustments.
Educating patients from the outset that modifications may be needed empowers them and prevents the perception of treatment failure.
Occlusal Equilibration Protocol: When TMD causes changes in jaw position, simple occlusal adjustments to posterior teeth can reestablish anterior contact without requiring restoration replacement.
This approach is far more efficient and cost-effective than attempting to prevent all future changes through initial restoration design.
Xerostomia and Cervical Decay: Severe dry mouth, whether medication-induced or from other causes, creates an extremely high-risk environment for cervical decay. Full-coverage crowns with margins that cover vulnerable root surfaces provide essential protection.
Conservative approaches like monitoring or small restorations are often inadequate in severe xerostomia cases.
Patient Autonomy in Treatment Planning: When adjunctive procedures (gum surgery, orthodontics) could improve outcomes but are not essential, patients should be fully informed of their options and empowered to make decisions based on their own priorities and tolerance for additional treatment.
Outstanding results can still be achieved when expectations are properly established.
Staging for Complex Cases: Separating maxillary and mandibular preparation into different appointments allows for more controlled occlusal development, particularly important in TMD patients, where jaw position may be unstable.
Comprehensive vs. Segmental Approach: In cases of severe xerostomia with multiple cervical lesions, comprehensive treatment protecting all tooth surfaces is often more appropriate than attempting to address individual teeth over time.
This case is appropriate for referral when patients present with active TMD requiring comprehensive restoration, severe xerostomia with multiple cervical cavities, failed restorative attempts at multiple practices, or complex cases requiring comprehensive prosthodontic rehabilitation with ongoing management.
Dr. Pytlik welcomes referrals for complex prosthodontic cases that require TMD management, treatment in high-decay-risk environments, and comprehensive rehabilitation, with realistic patient education and expectations.