How the Patient Found the Practice
Cecil found Dr. Pytlik’s practice through online reviews and a recommendation from his insurance company.
This combination of peer validation and professional endorsement reflects the trust that both patients and insurance providers place in specialized prosthodontic care for complex restorative cases.
Initial Condition & Life Before Treatment
The patient had lost his front teeth and had been provided with a removable partial denture to replace teeth in both his upper left area and his upper front area. Every single time the patient needed to remove the partial, he would be missing his front teeth.
The situation was extremely embarrassing to him, particularly when he had to remove the partial around family and friends.
This scenario highlights a common challenge with removable partial dentures: while they restore function and aesthetics when worn, they create significant psychological and social challenges when removed.
Unlike fixed restorations, removable partial dentures must be removed for cleaning and overnight wear, leaving patients without teeth during these times. For individuals missing anterior teeth, this creates predictable embarrassment and anxiety about being seen without their prosthesis.
The patient’s goal was clear: transition to a fixed prosthesis using bridges and implant restorations.
Fixed prosthodontics offers several advantages over removable options, including eliminating the psychological burden of tooth removal, improving stability during function, better preserving remaining tooth structure when properly designed, and enhancing long-term bone preservation when combined with implant support.

Pre-treatment retracted view with teeth separated, showing the extent of tooth loss and existing partial denture framework.

Post-treatment retracted view with teeth apart showing completed maxillary fixed bridge and crown restorations.
First Appointment & Discovery
During the first appointment, Dr. Pytlik recommended a full-mouth rehabilitation, treating both arches to idealize the patient’s bite.
This comprehensive approach would level the lower arch, which currently resembled a “roller coaster” due to years of uneven wear and tooth loss.
The treatment would prevent any occlusal interferences and, by increasing the vertical dimension, would help open the airway slightly more, addressing changes that had occurred from the bite closing over the years.
This comprehensive evaluation reflects the prosthodontic principle of examining the entire masticatory system rather than treating teeth in isolation.
When teeth are lost or worn unevenly, the remaining teeth often shift and over-erupt, creating an uneven occlusal plane. This “roller coaster” effect can lead to premature contacts, excessive wear on certain teeth, and compromised function.
Additionally, loss of vertical dimension (the height of the bite) commonly occurs with tooth loss and wear, which can contribute to TMJ issues and, in some cases, reduced airway space.
The patient understood all the recommendations and chose to proceed with just the upper arch initially. The patient also understood that a fixed bridge could not close both gaps in his occlusion simultaneously.
The patient recognized that a better implant site was available in his upper left area and chose to proceed with a fixed bridge in the anterior region, while planning implant placement in the posterior region.
This staged approach is common in complex prosthodontic cases, allowing patients to address their most pressing concerns first while maintaining a clear roadmap for completing comprehensive treatment.
Dr. Pytlik’s transparent discussion of ideal versus phased treatment options empowers patients to make informed decisions based on their priorities, timeline, and financial considerations.

Pre-treatment overhead view of maxillary arch showing removable partial denture in place with metal framework. Limited remaining natural teeth and extensive tooth loss requiring full arch rehabilitation.

Maxillary arch view with partial denture removed, revealing the extent of tooth loss in the anterior region. The missing central incisor and multiple gaps demonstrate significant aesthetic and functional deficits when the partial denture is out.
Misunderstandings or Clinical Oversights
In the maxillary anterior area, the final restoration replaces four teeth, making the bridge span relatively long.
However, these anterior teeth do not bear a significant occlusal load during function. In a properly designed occlusion, the anterior teeth primarily guide the jaw during lateral and protrusive movements while providing aesthetic support for the lips and face. The heavy chewing forces are borne by the posterior teeth.
A common misconception in dentistry is that all long-span bridges carry equal risk of failure. However, the location and function of the restoration significantly impact its prognosis.
Anterior bridges that replace multiple teeth can be highly successful when several factors are present: adequate abutment teeth with healthy periodontal support, proper distribution of occlusal forces (ensuring posterior teeth bear the brunt of chewing loads), excellent oral hygiene maintenance by the patient, and precise laboratory fabrication with proper pontic design.
The key clinical consideration in this case was to ensure that the anterior bridge would function primarily for aesthetics and guidance, rather than for heavy chewing.
By maintaining proper posterior occlusion and potentially adding posterior implant support in the future, the long anterior span becomes clinically predictable rather than risky.
Treatment Plan & Approach
The patient underwent maxillary arch rehabilitation, in which all maxillary teeth were prepared for crowns. This comprehensive approach allowed Dr. Pytlik to idealize the occlusion, correct the alignment of all upper teeth simultaneously, and create a cohesive aesthetic result.
Initially, the patient received maxillary temporaries for both the anterior and posterior regions.
This temporary phase served multiple critical functions: it allowed Dr. Pytlik to idealize occlusion and esthetics before committing to the final restoration, it created a blueprint of exactly what the final prosthesis would look like, and it gave the patient the opportunity to “test drive” the new bite and appearance.
Even though implants would eventually be placed in the maxillary left area, and the patient would need an interim partial as a temporary prosthesis during implant healing, Dr. Pytlik wanted the patient to understand what the final product would look like.
This visualization is invaluable for patient acceptance and satisfaction.
The use of provisional restorations in complex prosthodontic cases cannot be overstated. Temporaries allow the clinician to evaluate function, phonetics, and aesthetics before final fabrication.
They permit adjustments based on patient feedback. They also serve as a communication tool with the laboratory, providing a three-dimensional prescription of the desired final result.
After the maxillary prosthesis was completed, the patient understood that he needed to wear a night guard to prevent overloading of his anterior bridge.
Nocturnal bruxism (nighttime grinding or clenching) can place excessive forces on any restoration, but particularly on longer-span bridges.
A properly fabricated night guard protects both the restoration and the underlying tooth structure by distributing forces evenly and reducing the magnitude of parafunctional loading.
The patient also understood that he would transition to implant placement in the posterior region after the anterior bridge was completed.
The interim plan included fabricating a partial denture to be worn during the surgical healing phase after implant placement, as the patient was already accustomed to wearing a partial and preferred this familiar option during the healing period.

Overhead retracted view of completed maxillary arch rehabilitation showing comprehensive crown coverage and fixed anterior bridge.
Case Progression & Key Milestones
The patient appreciated the transparency, explanations, and the temporary phases he went through, which helped him fully understand what the final product would look like.
The treatment unfolded in clear stages, each building upon the previous phase.
The patient was particularly pleased that the temporary phase allowed him to see the final product in a provisional form.
This eliminated surprises and gave him confidence in the planned outcome. He was also able to help choose the color of his upper teeth, creating a sense of ownership and partnership in the treatment process.
One specific aspect the patient valued was maintaining the same esthetics he had previously, particularly the length of his front teeth, which created ideal lip support.
Rather than imposing a predetermined ideal, Dr. Pytlik worked with the patient to preserve the tooth proportions and lip relationships that felt natural and appropriate for this individual.
This patient-centered approach to aesthetics reflects an important principle in prosthodontics: the goal is not to create a “perfect” smile based on abstract ideals, but rather to restore function and confidence while respecting each patient’s unique facial proportions, preferences, and self-image. Lip support, tooth length, and facial harmony must be customized to each individual.
Treatment required two appointments for primary arch rehabilitation, plus two additional appointments to fabricate the partial denture, which would serve as an interim prosthesis during the implant-healing phase.
Outcome
Cecil achieved a stable, functional restoration of the maxillary arch with a long-span anterior bridge that effectively replaced the missing front teeth.
The fixed prosthesis eliminated the need to remove a partial denture daily in the anterior region, providing continuous tooth presence and function.
He was ready to proceed to an oral surgeon for implant placement in his upper left area, with full understanding of what the final implant-supported restoration would look like based on the completed anterior bridge.
During the surgical and healing phase, the patient would wear a partial denture, which he was already accustomed to using.
The comprehensive crown preparation of all maxillary teeth allowed for ideal occlusal adjustment and proper distribution of forces. The protection protocol of wearing a night guard was established to prevent excessive loading on the anterior bridge during nocturnal parafunction.
Cecil loved the esthetics of the bridge and how it supported his lip in a smile. The length and positioning of the anterior teeth created natural-looking facial support without appearing artificial or overdone.
His wife was actively involved in the decision-making process and was particularly pleased with the color selection she helped make.
Currently, Cecil appreciates that if he hasn’t placed his partial for any reason, or needs to remove it when he’s with family and friends or at home, he’s no longer embarrassed by missing teeth.
The fixed anterior bridge has eliminated the psychological burden of tooth removal in social situations.
This emotional relief represents one of the most significant benefits of transitioning from removable to fixed prosthodontics.
While both types of restorations can be fabricated to high esthetic standards, the permanence of fixed restorations provides psychological benefits that extend far beyond clinical function.
Patients no longer experience anxiety about their prosthesis becoming loose during eating or speaking, concern about being seen without their teeth, or the daily reminder of tooth loss that comes with inserting and removing a partial denture.

Natural repose photograph showing the patient's completed smile at rest with relaxed lip position.
Treatment Time
Treatment required two appointments for comprehensive maxillary arch rehabilitation, plus two additional appointments to fabricate the partial denture to be used during the implant healing phase.
This timeline reflects the phased nature of the treatment, with the fixed-bridge component completed relatively efficiently while planning for future implant restorations.
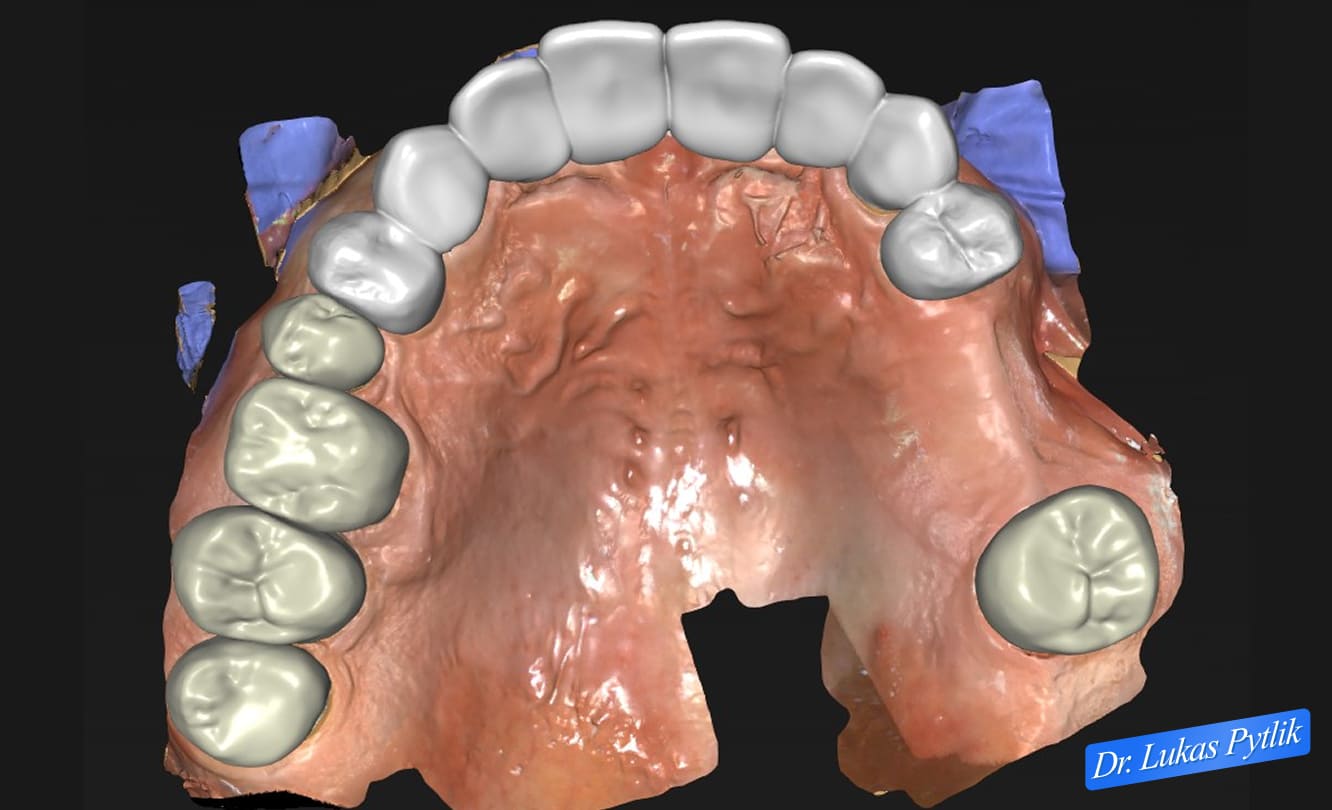
3D digital treatment planning showing an overhead view of the maxillary arch with proposed restoration design.
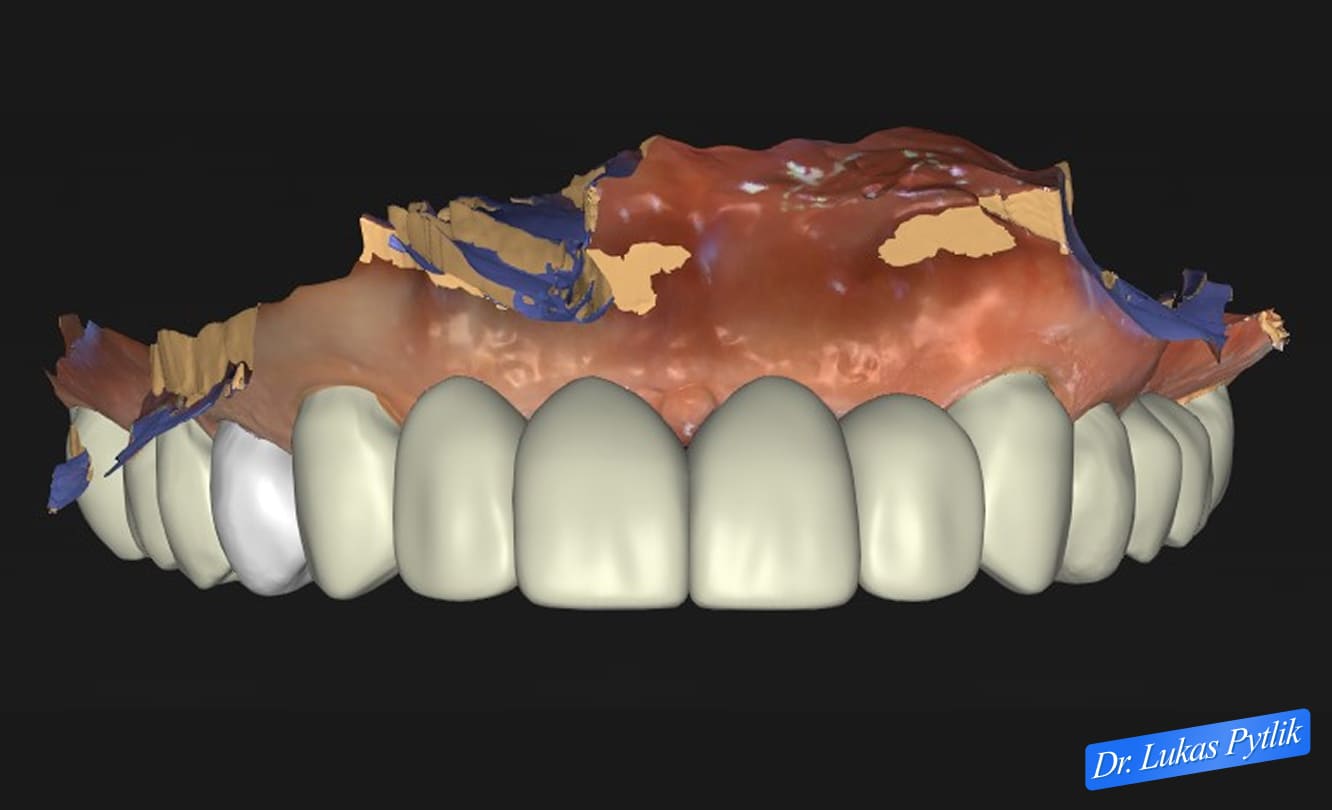
Digital design of provisional maxillary restorations in frontal view. Temporary phase design allows the patient to visualize and test the final outcome before definitive restoration fabrication, ensuring aesthetic approval and functional verification.
Clinical Notes for Referring Doctors
This case demonstrates the importance of comprehensive treatment planning with transparent patient education, even when treatment is completed in phases.
Dr. Pytlik’s approach to presenting the ideal comprehensive treatment (full-mouth rehabilitation) while respecting the patient’s decision to proceed with a phased approach created a collaborative environment and established realistic expectations.
Key clinical considerations in this case included:
Treatment Sequencing: By completing the maxillary arch rehabilitation first, Dr. Pytlik established proper occlusion and aesthetics in the upper arch before proceeding to implant surgery. This allowed the implant restoration to be designed to fit within an already idealized occlusal scheme.
Long-Span Anterior Bridges: The four-unit anterior bridge replacing multiple teeth was designed with the understanding that anterior teeth bear minimal occlusal load. Success factors include proper force distribution to posterior teeth, excellent abutment selection and preparation, and patient commitment to protective devices (night guard) and oral hygiene.
Provisional Restoration Phase: The use of comprehensive temporary restorations served multiple purposes: functional and aesthetic testing, patient communication and acceptance, laboratory prescription for final fabrication, and patient confidence-building through visualization of the final result.
Patient Empowerment: Dr. Pytlik ensured that the patient had a full understanding of treatment options, limitations, and sequencing. This transparency empowers patients to make informed decisions and holds them accountable for their role in treatment success, including maintaining hygiene and adhering to protection protocols.
Implant Planning: Rather than rushing to implant placement, the case was staged to allow the patient to experience the fixed restoration in the anterior region first. The posterior implant site was preserved for future definitive treatment, with an interim removable partial serving during the healing phase.

Digital scan showing completed case with final restorations in place. A comprehensive view demonstrates successful maxillary rehabilitation with proper occlusal relationships and preparation for future posterior implant placement.
This case is appropriate for referral when patients present with failing or poorly fitting removable partial dentures with aesthetic concerns, missing anterior teeth requiring fixed restorations, comprehensive maxillary rehabilitation needs, or staged treatment requiring coordination across multiple phases of care.
Dr. Pytlik welcomes referrals for complex prosthodontic cases requiring transitional restorations, comprehensive arch rehabilitation, and coordination of fixed and implant-supported prosthetics.